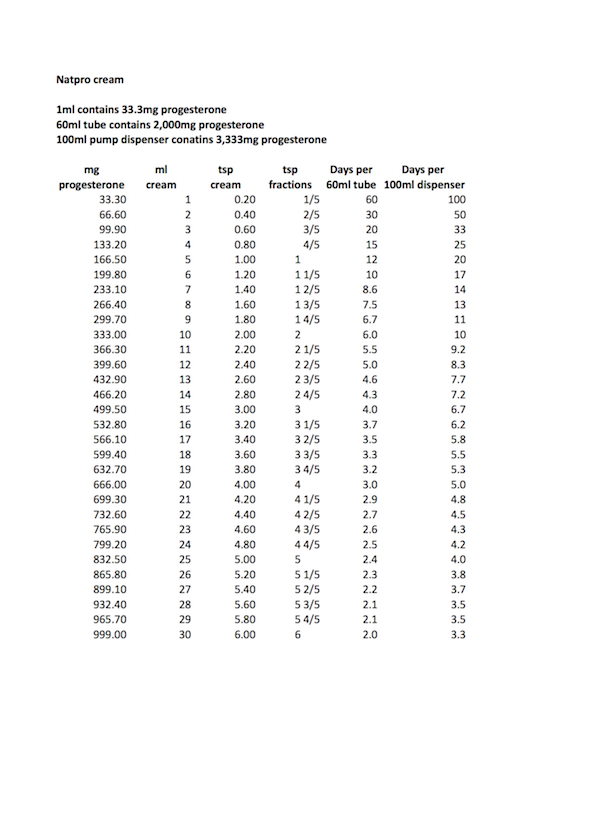
How to use progesterone to extend the luteal phase
A low dose of progesterone will not help. 100-200mg/day or more progesterone should be used, depending on symptoms. In some cases up to 400mg/day will be needed. It should be used from ovulation, or during the 50 hour pre-ovulatory surge.
If used too early i.e. 7 to 8 days before ovulation, which is when many women are told to start it, progesterone can act as a contraceptive, but usually 200mg/day or more are needed. So starting too early can prevent the chance of falling pregnant.
When to start using progesterone
It is advisable to start the progesterone well before pregnancy to allow the body to adjust. Many women are started on progesterone many days, often weeks after they fall pregnant and suffer oestrogen dominance symptoms. It's bad enough suffering from these when first pregnant, but twice?! For more info please see the page on Oestrogen Dominance.
How to check when ovulation has occurred
Taking temperature readings or using a mini microscope will help to check for ovulation, the mini microscope is more reliable, as temperature can vary from as little as 0.5 degrees to 5 degrees.
Saliva or vaginal mucus is used for the test, by dabbing a small amount on the end of the microscope. During the follicular phase, the pattern formed by the saliva/mucus is spotty, as ovulation draws near a fern like pattern starts emerging, becoming completely fern like when ovulation has occurred, returning to the spotty pattern almost immediately. For more information see Ovulation Microscope.
Normal oral body temperature in adult men and women ranges between 33.2-38.2°C (92-101°F). Typical average temperatures are 37.0°C (98.6°F).
In women it varies between the follicular and the luteal phase. During the follicular phase, i.e. from the first day of menstruation to ovulation, it ranges from 36.45 to 36.7°C (97.6 to 98.1°F).
During the 12-14 day luteal phase, i.e. after ovulation to menstruation, temperature increases by 0.15 - 0.45°C (0.2 - 0.9°F) due to the increased metabolic rate caused by rapidly rising levels of progesterone. Temperature ranges between 36.7 - 37.3°C (98.1 - 99.2°F) during the luteal phase, but drops down to follicular levels within a few days of bleeding.
Fertilisation
One of the most important things to remember about conception is the life span of the sperm and ovum. The average life of the sperm appears to be two to three days, sometimes longer, but the ovum only lives twelve hours and in rare cases twenty four hours.
All research points to a greater success in conception if intercourse takes place in the one to two days prior to ovulation, when the fern like pattern is almost complete. This is during the preovulatory progesterone surge.
This allows time for the sperm to travel through the uterus and up the Fallopian tubes to meet the egg before it becomes over mature or it dies. One of the problems with an over mature egg is it diminishes the chances of fertilisation, can result in a miscarriage or result in foetal abnormalities. The health of the future child is dependant on these factors.
The nearer intercourse takes place to ovulation, the greater the chances of conception.
Pregnancy
It must be remembered that twelve to fourteen days is necessary for the lining to mature enough to receive a fertilised egg. If bleeding does occur, it means the egg has not been fertilised or implantation has not taken place. The progesterone should then be stopped and only started again at the next ovulation. If bleeding does not start fourteen days later, it is possible that fertilisation and implantation have occurred.
On no account must the progesterone be stopped at this stage, otherwise it could cause a miscarriage.
If there is no menstruation and pregnancy is confirmed, the progesterone should be continued, using between 100-200mg/day or more until the fourth month. After the critical stage has passed the progesterone it can be tapered off slowly, or can be continued until birth.
The majority of women are advised to stop cold turkey, this is not advisable. Progesterone withdrawal can not only cause a miscarriage if the placenta is making insufficient at this point. But other adverse symptoms can occur. These are the same as those experienced due to progesterone withdrawal the few days prior to bleeding during the monthly cycle.
If tapering off, the amount should be reduced very slowly, taking about a month to do so. This is easy to do if using a progesterone cream, difficult if using injections or suppositories. Either switch to a cream, or in the case of injections withdraw slightly less progesterone from the vial for each reduction. In the case of suppositories, divide them into 25mg pieces, adjusting the tapering by using as many pieces as required.
It's advisable to continue using progesterone until birth if there's a likelihood of a pre-term birth or pre-eclampsia.
Please monitor symptoms, and if spotting, headaches, water retention or nausea should occur increase the amount and continue using it till birth. In some women water retention and a rise in blood pressure sometimes occurs in the last one to two months, please increase the amount if this should happen.
If nausea occurs 400-800mg/day is needed to stop it.
It is the first three, possibly four months that are critical. 25% of miscarriages occur during the first six weeks when the child is still in the embryo stage. The risk drops to 8% after eight weeks, when the child is now termed a foetus.
During this time the placenta is developing and after about two months starts secreting progesterone, while ovarian production starts declining. If at this point placental production is insufficient to meet the demands of the growing foetus a miscarriage can occur. It is therefore advisable to continue with the supplemental progesterone until at least the third month. All being well the placenta continues to make progesterone in increasing amounts until birth, when levels drop abruptly with the expulsion of the placenta, or afterbirth as it's now generally termed.
Miscarriages and Pre-term births
Many factors cause miscarriages, far too many for here. But a few are chromosomal alterations, uterine anomalies, antiphospholipid antibodies, exposure to bisphenol A an endocrine disruptor, high alcohol intake, high levels of the inflammatory cytokines TNFa and IL-6, and natural killer cells, if activated by TNFa, may cause the death of the embryo. Progesterone suppresses TNFa and IL-6 activity, and excessive NK cell activity.
Of significance for this page are low levels of progesterone and Vitamin D, and high levels of oestrogen and free testosterone, often overlooked. A level of progesterone over 12.3 ng/ml in early pregnancy indicates a normal pregnancy.
A ratio of 1.05 or higher for free testosterone to total testosterone indicates a miscarriage is likely. But if the free testosterone ratio is lower than 0.84 a normal pregnancy occurs. The reasoning behind this is excess oestrogen causes foetal death. The enzyme 5-alpha reductase Type 1 mRNA is induced in the pregnant brain, this inactivates testosterone, which reduces the available substrate for oestrogen synthesis.
Progesterone also inhibits the enzyme aromatase, which effects the conversion of testosterone to oestrogen.
A short cervix increases the risk of pre-term births, progesterone reduces the risk.
It is also essential to bear in mind that stress can cause a miscarriage. The rise in cortisol in response to the stress, results in a drop in the progesterone level, this in turn can lead to spotting or a miscarriage. To prevent this, as soon as any stress is felt, increase the amount of progesterone till it has passed. If any Anxiety is felt please look through this page.
Many women are devastated by a miscarriage, understandably, but none are warned that as many as 20% of all pregnancies end in a miscarriage within two weeks of fertilisation. Another 15% occur within the first fourteen weeks (three and half months).
A short cervix increases the risk of pre-term births, progesterone reduces the risk.
It is also essential to bear in mind that stress can cause a miscarriage. The rise in cortisol in response to the stress, results in a drop in the progesterone level, this in turn can lead to spotting or a miscarriage. To prevent this, as soon as any stress is felt, increase the amount of progesterone till it has passed. If any anxiety is felt please look through this page.
Many women are devastated by a miscarriage, understandably, but none are warned that as many as 20% of all pregnancies end in a miscarriage within two weeks of fertilisation. Another 15% occur within the first fourteen weeks (three and half months).
Preeclampsia
Studies have shown that low progesterone and vitamin D levels are found in preeclampsia. One study finding progesterone was 'pathologically and statistically' lower. Serum allopregnanolone (a potent metabolite of progesterone) was found to be significantly lower too. The Th1 (inflammatory cytokines) and Th2 (anti-inflammatory cytokines) play a role. The number of Th1 cells and the ratio of Th1:Th2 in preeclampsia is significantly higher than in a normal pregnancy. Progesterone and vitamin D both increase levels of Th2.
But a number of other factors have been found to play a role. Women with insulin resistance, high levels of malondialdehyde and homocysteine are at greater risk of developing preeclampsia. A lack of selenium and low levels of glutathione and other antioxidants increase the risk too.
If recurrent miscarriages, pre-term births or preeclampsia have occurred consider using 200-600mg/day progesterone. Many believe progesterone is not effective at preventing these, but the evidence points to far too little progesterone being used in the unsuccessful studies.
Depression
25% of women suffer some form of depression after child birth. From the 'baby blues', to post natal depression (PND), to post natal psychosis (PNP), which can result in infanticide and suicide. Luckily PNP only occurs in 0.05% of women. The depression is caused by the rapid drop in progesterone levels after the expulsion of the placenta. Serotonin levels drop too. Anti-depressants are not required, what is are large amounts of progesterone. From 800mg/day for PND up to 2400mg/day for post natal psychosis, the amounts Dr Dalton found effective.
To recap...
Progesterone must only be used at ovulation, or during the 50 hour preovulatory surge if pregnancy is the aim
Take temperature readings or use a mini microscope to help check for ovulation
On no account must the progesterone be stopped if conception is suspected, otherwise it could cause a miscarriage
It is essential to continue the progesterone over the first 2-3 month critical phase, particularly the first 2 months
It is also essential to bear in mind that stress can cause a miscarriage
The nearer intercourse takes place to ovulation, the greater the chances of conception
Use at least 100-200mg/day progesterone, possibly more
It should always be used a minimum of twice a day by dividing the amount
Make sure sufficient nutrients are taken to support the pregnancy, particularly vitamin D and taurine
Avoid all skin care, foods and drinks which contain endocrine disruptors and other toxins, these can cause epigenetic changes in the foetus
Drugs
Mention should be made of the drugs which are often given in place of progesterone to prevent miscarriages and pre-term births, in the mistaken belief they are one and the same. One is a synthetic progesterone called Duphaston which contains dydrogesterone. Another is 17-hydroxyprogesterone caproate (17-OHP-C), also a synthetic hormone.
But because they're progestins, they are not broken down into the normal progesterone metabolites, such as the all important allopregnanolone. These are as essential as progesterone itself, especially in pregnancy, when the foetus is particularly susceptible to toxins or a lack of necessary nutrients.
A metabolite of progesterone is sometimes used too, 17-Hydroxyprogesterone, this is natural, and increases during the third trimester. It's often called 17-OHP, or 17-OH, or 17-P.
No adverse side affects have been reported with the use of 17-OHP, which is produced primarily by the adrenal glands. But there are safety concerns about 17-OHP-C use. Progesterone is also more potent that 17-OHP-C.
OTC Drugs
Many women take over-the-counter mild analgesics during pregnancy. Drugs such as acetaminophen (paracetamol), and non-steroidal anti-inflammatory drugs (NSAIDS) like ibuprofen and acetylsalicyclic acid (aspirin). These have been shown to increase the risk of congenital malformations, including cryptorchidism and hypospadia. Paracetamol in particular increased the risk of cryptorchidism as it's a potent inhibitor of androgen production.
hCG
hCG or human chorionic gonadotrophin is a hormone produced by the developing embryo after conception. Once the embryo has implanted a specialised part of the placenta takes over production. The role of hCG is to prevent the corpus luteum from disintegration. The corpus luteum is critical for the production of progesterone for the first 8 weeks, until the placenta begins to take over production. Please note that hCG starts dropping after 13 to 16 weeks GA as the corpus luteum is no longer needed.
GA: Gestational Age or LMP: Last Menstrual Period
It is standard practice to take the last menstrual period as the 'age' of the foetus. This is always regarded as occurring 14 days prior to ovulation. But foetal age can of course vary, as the menstrual cycle varies between 21 to 35 days. Ovulation occurring between days 7 to 21, and therefore conception occurring on or just after. If a woman has a longer or shorter cycle than 28 days, this should be taken into account.
Chart taken from Dr Dalton's book "Once a Month"...
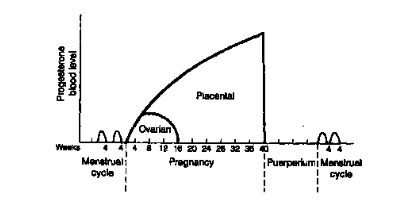
Levels of progesterone during the menstrual cycle and pregnancy
Here's the link to the chapter from Dr Dalton's book 'PMS The Essential Guide to Treatment Options' on the role progesterone plays during pregnancy.
In memory of Dr Katherina (Kittie) Dalton.
To understand the hormonal changes in pregnancy please see the page on Hormone Testing.
Additional information
The growing foetus is an extra burden on the mother, so it is essential to make sure all nutrients the foetus needs are available.
Please consider taking the following each day...
5 000iu's/day vitamin D3 (cholecalciferol) vital for a developing foetus, to prevent miscarriages, epigenetic changes, rickets, heart failure, epilepsy, Type 1 diabetes, and upper respiratory track infections in the newborn, to reduce the risk of preeclampsia in the mother
1000-2000mg/day taurine to prevent epilepsy, insulin resistance, impaired glucose tolerance, diabetes, impaired neurological function, vascular dysfunction and growth retardation in the developing foetus and newborn. Taurine is not found in grains, legumes, vegetables, nuts, seeds or fruit, only animal protein.
5ml Omega 3 fish oil, particularly DHA, needed by the developing brain
Vitamin B complex with extra folic acid bringing this up to 800mcg/day to prevent neural tube defects. If a vegetarian, please be cautious, as excess folic acid masks a B12 deficiency. A lack of B12 in utero increases the risk of insulin resistance in the child.
Do not take cod liver oil, or any fish liver oil. The excessive vitamin A it contains prevents vitamin D from being absorbed. Take beta-carotene if short of vitamin A.
To clear any confusion, 'fish oil' comes from the muscle of the fish and contains Omega 3. Fish 'liver' oil obviously comes from the liver, it contains large amounts of vitamin A and very small amounts of vitamin D. There is a world of difference between the two.
For more info on vitamin D levels, test kits etc see...Vitamin D Council
GrassrootsHealth
Birmingham Hospital
Vitamin D Links
Blood levels should be 70-100ng/ml (175-250nmol/L) and not the 30ng/ml (75nmol/L) most labs and doctors regard as adequate. The minimum daily dose should be 5000iu's per day, although recent research indicates it should be 10,000iu's per day, see here.
Read all labels on containers, especially those for food and cosmetics. Look for natural alternatives to body care products, many contain high levels of endocrine disruptors and carcinogens, particularly the sunscreens.
Please see Our Stolen Future for more information on endocrine disruptors.
Please see the page on Nutrition for more information about food.
For more information on pregnancy see..
Read more: http://www.progesteronetherapy.com/faq-conception.html#ixzz2DYkYi1QT
Under Creative Commons License: Attribution